Download
1 / 48
530 likes | 900 Views
Kirstin Blackie Nima Mohan. Medical Abdomen. Be aware of common conditions presenting with abdominal symptoms Understand important factors in the history, examination, investigation and management of common abdominal pathologies. Objectives. Causes of Abdo Pain.
 elani
elani

E N D
Kirstin Blackie Nima Mohan Medical Abdomen
Be aware of common conditions presenting with abdominal symptoms • Understand important factors in the history, examination, investigation and management of common abdominal pathologies. Objectives
Causes of Abdo Pain
Mr C, 35 year old man, presents to his GP with mild abdominal pain and yellowing of the whites of his eyes (noticed by his girlfriend who is a nurse). • What other symptoms would you want to ask about? Case Study
Abdominal pain (RUQ) • Jaundice • Nausea, vomiting Weight loss • Abdo distension • Haematemesis and malaena • Breast swelling, tesicular atrophy • Confusion • Spider naevi • Palmar erythema • Dupuytrens contracture • Hepatomegaly, Spenomegaly Signs and Symptoms of Liver pathology
Has recently has ‘flu’ – has felt generally unwell, tired and vaguely nauseated. He is unsure but thinks he may have had a mild fever. • What risk factors would you ask about? Case study cont:
High Alcohol intake • Blood-to-blood contact (IVDU, Tattoos, infected transfusions, needlestick injuries) • Unprotected sex • Drugs (prescribed, OTC, herbal) • Travel • Family history of liver disease (autoimmune hepatitis, Wilson’s disease) Mr C is in monogamous sexual relationship with girlfriend for 2 months– she is on OCP. No barrier contraception. Drinks approximately 30 units alcohol / week. Denies any other risk factors. • What first line investigations would you like to do? Risk factors for liver disease
Viral hepatitis: • ALT greatly raised (10-100x upper limit of normal) • Alcoholic hepatitis • ALT moderately raised (2-10x upper limit of normal) • Drug induced hepatitis • Mixed picture: raised hepatic (AST, ALT) and Cholestatic (Alk Phos and GGT) markers Abnormal clotting (prolonged PT or INR) may indicate acute liver failure Liver Function Tests
Acute hepatocellular damage: • Paracetamol (dose related) • Alcohol (dose related) • TB drugs • Anticonvulsants • Azathioprine • Methotrexate • Chronic active hepatitis • Nitrofurantoin • Isoniazide • Intrahepatic cholestasis • Azathioprine • Oestrogens • erythromycin Drugs commonly associated with Hepatitis
Other causes: EBV, CMV, paravirus B19, dengue, yellow fever.
Hepatitis E endemic areas
Girlfriend • Mr C Mr C and his girlfriend are both tested for viral hepatitis
Hepatitis B Serological Markers
What are the differential diagnoses? 65 year old man who hasn’t been to his GP in years comes into A+E with an uncomfortable swollen abdomen
Fat • Faeces • Fluid • Foetus • Flatus How would you examine for fluid (ascites)? 5 Fs of distended abdomen
Shifting Dullness Does the presence of ascites prove that this patient has liver disease?
What are the possible causes of ascites?
Alcohol excess • Hepatitis B • Hepatitis C • Non-alcoholic Fatty Liver disease / Non-alcoholic Steatohepatitis • Haemachromatosis • Primary Biliary Cirrhosis • Primary Scelosis Cholangitis • Autoimmune hepatitis • Wilson’s disease and other inherited metabolic disorders Cirrhosis: common end point of many disease processes
Bloods: likely increased biliruben, AST, ALT, alk phos, GGT; Decreased albumin, increased PT/INR (reduced synthetic function); Decreased WCC and platelets (hypersplenism); Look for the cause: serology, autoantibodies, iron studies Imaging: liver US and doppler, MRI Ascitic tap: Biopsy: confirm clinical diagnosis How would you investigate decompensated liver disease?
“fibrotic, structurally abnormal nodules in liver …. Compatible with cirrhosis. Doppler shows signs of portal hypertension.” US liver
Anaemia (folate deficiency, hypersplenism) • Thrombocytopenia (hypersplenism) • Coagulopathy (reduced production of clotting factors) – can lead to DIC • Oesophageal varices • Spontaneous Bacterial Peritonitis • Hepatic encephalopathy • Hepatocellular carcinoma Complications of Cirrhosis
Patient education and support • Treat underlying cause • Adequate nutrition (calorie and protein intake) • Careful prescribing • Therapeutic ascetic tap • Alcohol abstinence (also important in non-alcohol induced cirrhosis) • Alcohol dependent individuals will require: Chlordiazepoxide, Thiamine, Vitamin B • Monitoring for further complications: • oesophageal varicies or HCC • ?transplant How would you manage this patient?
“A 17 year old girl presents to the GP with a 8 week history of fatigue. She also reports frequent episodes of pyrexia and intermittent episodes of diarrhoea over this period. Over the last 48 hours she has had 14 episodes of watery diarrhoea” What other questions would you askher??? Case Study
She denies...... • jaundice, dyspepsia, vomiting, malena, constipation, ulcers • Changes in appetite • Changes in mensustral cycle • urinary symptoms • No recent travel • No changes / alterations to her diet She reports ....... • Fatigue – low energy levels • SOBOE • Palpitations • Frequent Pyrexia • Abdominal pain – generalised cramps • Diarrhoea – no blood or mucus • Weight Loss
Clinical Examination • Investigations Urine Dip and MSU Bloods : FBC, U&E's , CRP, ESR, LFT's, TFT's, Electrolytes, Anti -TTG, Blood Cultures?? Stool culture • Imaging What are you going to do next??
Clinic On examination ...... • Tachycardic – 101 regular, good volume. • normotensive – 110/76 • CPT > 3 sec • Pale conjunctive • Cardio- respiratory examination - NAD • Diffuse tenderness in the abdomen • normal PR What is your immediate management plan?
WHAT TYPE OF IMAGING?NAME OF SIGN?WHAT DISEASE? 5 OTHER EXTRA INTESTINAL MANIFESTATIONS OF THIS DISEASE?
EXTRA INTESTINAL MANIFESTATIONS • EYES : episcleritis, uveitis • MOUTH: Apthous ulcers, angular stomatitis • JOINTS : sero-negative arthropathies (anklysing spondylitis, sacroilietis) • KIDNEYS : stones fistula, hydronephrosis • SKIN: Eryhthemna nodosum, phlebitis, pyoderma gangrenosum
Clinic
Strongly association with UC (less with CD) • Inflammation, fibrosis and stricture of the intra/ extra hepatic ducts. • Signs of Live failure • LFTS- Raised Alkaline Phosphatase, Bilirubin, hypergamaglobinumina • ANA, ANCA, SMA +VE • Poor prognosis – often need transplant and increases risk of cholangiocarcinoma Primary Sclerosing Cholangitis
MEDICAL MANAGEMENT Treatment of exacerbations : • Mild – oral steroids (Prednislone PO / PR) • Severe – IV Hydrocortisone and Antibiotics Maintenance therapy : • Maintain adequate nutrition • To prevent exacerbations • 5-ASA's (Mesalazine) • Azothioprine • Anti- TNF antibodies (INFLIXIMAB) Management
Surgical management of complications • Surgical management of the condition Surgical Management
A 25 year old girl presents with a 8 week history of generalised abdominal cramps and diarrhoea. They are loose stool, no blood or mucus and can occur 8-10 times a day. She also reports that she is frequently tired and stressed. • What else do you want to know??? CASE STUDY
Incidence: common (female 20 -40) ; 40 % people attending secondary care 6 months of symptoms before diagnosis Can be predominantly constipation or predominantly diahorrea. Abdominal pain/ Bloating Anxiety / depression Incomplete emptying/ incontinence/ urgency Constitunal symptoms : tiredness, lethargy, arthalgia, urinary symptoms, dyspurunina. RED FLAG SYMPTOMS: Bleeding, Nocturnal symptoms, weight loss, Age > 50 Irritable bowel Syndrome
Reassurance and support Address / Treat underlying medical issues Lifestyle advice : • Dietary modification – excluding food groups. • Smoking and alcohol Symptomatic relief : • Bloating – Peppermint oil • Constipation – increase fibre and fluid intake • Antispasmodics – mebevrine Treatment Options
“A 65 year old man presents with a 4 day history of black tarry stools. He reports that they are becoming more frequent and loose. He also reports nausea and one episode of vomiting this morning. He also reports that he has a back ache for the past fortnight and has been taking OTC painkillers for it and would like you to prescribe some more” Case Study
Common causes: • Ulcers – Peptic ulcers (40%) • Varices – Secondary to portal hypertension (17%) • Gastritis / gastric erosion • Duodenitis • Oesphagitis Rarer causes: • Mallory -Weiss tears • Angiodysplasia • Bleeding Disorders • Peutz- Jeugher's Syndrome • Osler – Webb – Rendu Syndrome Causes of Upper GI bleeding
On Examination: • He is tachycardic, at 111 bpm / regular and borderline hypotensive 105/72. • He is tender in the epigastrium and peri-umbilically. There is some voluntary guarding. Bowel sounds are normal. • DRE – Malodorous black tarry stool. No fresh blood. Investigations: • Bloods : Hb -10.0 , Urea -21 , Creatnine 66, WCC- 7.0, platelets- 260, CRP – 2.2, LFT's – NAD. • AXR – NAD • Erect CXR – No free air under the diapgram Examination / Investigation
Bleep : RR -30 BP- 90 /66 , HR -122, CRT > 3, Sats – 94% • A - No airway compromise • B – O2, ABG • C – IV access + Fluid Challenge (which??), Bloods. IV PPI, erect CXR, AXR • D – GCS, Pupils , Glucose • E - everything else: check notes, CALL FOR HELP RE- ASSESS Management
Pre-scope score : predicts the morbidity and mortality • Post -scope score : predicts the risk of re-bleeding Rockall Score
This is a sign of decompensation • ABC approach • IV Terlipressin (+ \ - Propanalol) • Clotting abnormality – correct it • Octreotide ( often given by seniors) • Secondary prevention (propanolol) • ABC approach • IV PPI • Endoscopy: CAUTERISTION or CLIPPING of the ulcer Bleeding secondary to varicies Bleeding secondary to ulcers
Sengstaken Blakemore Tube : Balloon Decompression • TIPS : Trans-jugular intrahepatic porto systemic shunt Management of Variceal Bleeding
A catheter into the hepatic vein, guidewire was passed into a portal vein branch. The tract was dilated with a balloon, and contrast injected. A metallic stent placed over the wire TIPS
THANK YOUANY QUESTIONS??

ABDOMEN. Lu Xiaoli Regional Anatomy & Operative Surgery China Medical University . BOUNDARIES . Abdominopelvic Cavity Abdominal Cavity Pelvic Cavity. P242-fig.4.21. DIVISIONS. P242-fig.4.22. P243-fig.4.23. P243-fig.4.23.
3.17k views • 93 slides
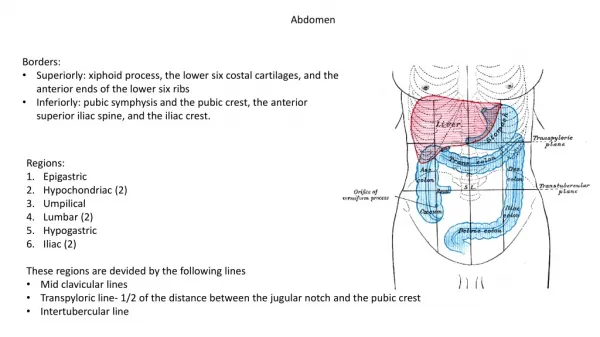
Abdomen. Borders : Superiorly: xiphoid process, the lower six costal cartilages, and the anterior ends of the lower six ribs Inferiorly: pubic symphysis and the pubic crest, the anterior superior iliac spine, and the iliac crest. Regions: Epigastric Hypochondriac (2) Umpilical Lumbar (2)
2.11k views • 61 slides
Abdomen. Adapted from Mosby’s Guide to Physical Examination, 6 th Ed. Ch. 17. Tips…. Perform early in the exam Relaxation and quiet Bottle/pacifier/nursing On parent’s lap Dr. sits facing the parent, knees touching. Ticklish?. Firm touch Place the child’s hand under your palm
832 views • 62 slides
Abdomen. Muscles of abdominal wall. Rectus abdominus--vertical midline Three layers form tube External oblique (“hands-in-pocket”) Internal oblique (fibers perpendicular to external) Transverse abdominus (wraps around). Muscles of abdominal wall--details. External Oblique.
730 views • 35 slides
ABDOMEN. The abdomen is the posterior end of the three body regions of an adult insect. It is composed of 11 segments. The abdomen bears the external genitalia of the insect. In female insects these consist of an ovipositor .
1.93k views • 17 slides
Abdomen. Abdomen. Abdomen is the part of the trunk between the thorax and pelvis.
535 views • 21 slides
ABDOMEN. 1. Abdominal bruits may indicate: Renal Stone Pancreatitis Aortic Aneurysm Ulcer. 1. Abdominal bruits may indicate: Renal Stone - colic quality Pancreatitis - knifelike; epigastric Aortic Aneurysm Ulcer - burning pain.
814 views • 57 slides
MEDICAL CAUSES OF THE ACUTE ABDOMEN. Dr. T.H De Klerk Critical Care 12 May 2014. DEFINITION. The term, acute abdomen, is the medical slang word that denotes an acute, serious abdominal condition, usually treated best by surgical operation.
733 views • 21 slides

Abdomen. Inspection : Distention Scaphoid Visible peristaltis Umbilical abnormalities Distended bladder. Shifting dullness fluid wave. Palpation: Tenderness Guarding Tumor Liver
668 views • 27 slides

ABDOMEN. Infection. Infection:. Appendicitis Diverticulitis Perinephric Abscess Renal Abscess. APPENDICITIS. Description:. Appendicitis is the inflammation of the vermiform appendix due to an obstruction. Appendicitis is the most common acute surgical condition of the abdomen. Etiology:.
1.79k views • 141 slides

abdomen. AP Abdomen. Naso-gastric (NG tube). Iodonated contrast in Left kidney. Inferior vena cava filter. AP View UGI. Oblique View UGI. Small Bowel Follow Through (Early). Ligament Of Treitz. Duodenal c-loop. Jejunum. Pancreatic head. Small Bowel Follow Through (1 hour later).
544 views • 31 slides
Abdomen. Professor Ravi Kant MS FRCS (Edin) FRCS (Glasg) FAMS FACS DNB FICS FAIS. MCQ. Short story = clinical vignette One line question 5 options= distractors One will be correct Blue print. Blue print. 10 basics = trauma 10 H&N 10 Breast 10 hernia, etc 10 jaundice, abdomen
537 views • 37 slides
ABDOMEN. Hepatobiliary. Hepatobiliary :. Cavernous Hemangioma Choledochal Cysts Choledocholithiasis Fatty Infiltration of the Liver Focal Nodular Hyperplasia Homochromatosis Hepatic Adenoma Hapatic Cysts Hepatic Metastases Hepatoma. CAVERNOUS HEMANGIOMA. Description:.
1.46k views • 118 slides

ABDOMEN. Gastrointestinal. Gastrointestinal:. Carcinoid Colorectal Cancer Crohn Disease Free Intraperitoneal Air Gastric Carcinoma Intussusception Ischemic Bowel Large Bowel Obstruction Mesenteric Adenitis Mesenteric Ischemia Small Bowel Obstruction Volvulus. CARCINOID.
1.37k views • 132 slides
ABDOMEN. Infection. Infection:. Appendicitis Diverticulitis Perinephric Abscess Renal Abscess. APPENDICITIS. Description:. Appendicitis is the inflammation of the vermiform appendix due to an obstruction. Appendicitis is the most common acute surgical condition of the abdomen. Etiology:.
1.48k views • 141 slides

ABDOMEN. Hepatobiliary. Hepatobiliary :. Cavernous Hemangioma Choledochal Cysts Choledocholithiasis Fatty Infiltration of the Liver Focal Nodular Hyperplasia Homochromatosis Hepatic Adenoma Hapatic Cysts Hepatic Metastases Hepatoma. CAVERNOUS HEMANGIOMA. Description:.
1.37k views • 118 slides
Abdomen. Anatomy of the Abdomen. Anatomy of the Abdomen (Abdominal Cavity). Four Quadrants. Midsternal line from the xiphoid process through the umbilicus to the pubic bone Horizontal line perpendicular to the first line through the umbilicus Quadrants named Right upper quadrant (RUQ)
477 views • 34 slides
ABDOMEN. Anatomical landmark in clinical exploration of the abdomen. What is normal?. Bony landmarks. Lower ribs Spine Iliac bone Inguinal ligament Pubic bone Sacrum – pelvic aperture. Anatomic landmarks. Xifoid apendix Costal margins Spina iliaca antero-superior Simphisis pubis
778 views • 65 slides
玻璃钢生产厂家橡胶玻璃钢牛雕塑制作沈阳华硕玻璃钢雕塑上海仿铜玻璃钢雕塑生产厂家常用玻璃钢花盆市场西安环保玻璃钢雕塑优势东莞玻璃钢鱼雕塑工厂东营神像玻璃钢雕塑金昌大型玻璃钢雕塑玻璃钢白胚雕塑释迦牟尼玻璃钢雕塑图片武穴玻璃钢花盆花器江苏通道商场美陈现价玻璃钢仿真动物雕塑厂家宁波市玻璃钢雕塑工程公司无锡镜面玻璃钢雕塑价格四川喷泉雕塑玻璃钢三门峡标识标牌校园玻璃钢雕塑玻璃钢景观雕塑培训湖南定制玻璃钢雕塑玻璃钢雕塑上什么漆玻璃钢雕塑鞋带忻州玻璃钢雕塑定制价格广东特色商场美陈销售厂家商场美陈户外门头玻璃钢造型雕塑用什么上色河南镜面玻璃钢仿铜雕塑定做沈阳玻璃钢雕塑制品茂名玻璃钢广场雕塑湖北景区玻璃钢雕塑批发邳州商场春季美陈香港通过《维护国家安全条例》两大学生合买彩票中奖一人不认账让美丽中国“从细节出发”19岁小伙救下5人后溺亡 多方发声单亲妈妈陷入热恋 14岁儿子报警汪小菲曝离婚始末遭遇山火的松茸之乡雅江山火三名扑火人员牺牲系谣言何赛飞追着代拍打萧美琴窜访捷克 外交部回应卫健委通报少年有偿捐血浆16次猝死手机成瘾是影响睡眠质量重要因素高校汽车撞人致3死16伤 司机系学生315晚会后胖东来又人满为患了小米汽车超级工厂正式揭幕中国拥有亿元资产的家庭达13.3万户周杰伦一审败诉网易男孩8年未见母亲被告知被遗忘许家印被限制高消费饲养员用铁锨驱打大熊猫被辞退男子被猫抓伤后确诊“猫抓病”特朗普无法缴纳4.54亿美元罚金倪萍分享减重40斤方法联合利华开始重组张家界的山上“长”满了韩国人?张立群任西安交通大学校长杨倩无缘巴黎奥运“重生之我在北大当嫡校长”黑马情侣提车了专访95后高颜值猪保姆考生莫言也上北大硕士复试名单了网友洛杉矶偶遇贾玲专家建议不必谈骨泥色变沉迷短剧的人就像掉进了杀猪盘奥巴马现身唐宁街 黑色着装引猜测七年后宇文玥被薅头发捞上岸事业单位女子向同事水杯投不明物质凯特王妃现身!外出购物视频曝光河南驻马店通报西平中学跳楼事件王树国卸任西安交大校长 师生送别恒大被罚41.75亿到底怎么缴男子被流浪猫绊倒 投喂者赔24万房客欠租失踪 房东直发愁西双版纳热带植物园回应蜉蝣大爆发钱人豪晒法院裁定实锤抄袭外国人感慨凌晨的中国很安全胖东来员工每周单休无小长假白宫:哈马斯三号人物被杀测试车高速逃费 小米:已补缴老人退休金被冒领16年 金额超20万